Next Article
The Microbiome’s Answer to Why Dieting Doesn’t Always Work
7 minutes
A 1984 study painted a shocking picture of how our gut protects us (or doesn’t) from dietary mercury. After nearly 40 years, we’re finally ready to understand the radical implications of this foundational research.
You might already know that mercury is bad for you. You might even know that, like many other heavy metals, it’s specifically bad for your brain.
This awareness goes back centuries, and is evident in cultural artifacts like Alice in Wonderland. The character of the Mad Hatter supposedly owes its existence partly to the use of mercury salts in hat-making, back in Victorian-era England—although the reality of the syndrome was less like the character’s zany antics, and instead a litany of symptoms like fatigue, anxiety, shyness, and irrational irritability that tended to wreck relationships.
As a society, we’ve done a pretty good job reducing people’s exposure to this toxin (part of why old-school thermometers containing the metal were phased out decades ago), but exposure to small amounts in food is still inevitable. Mercury is found at trace concentrations in soil and seawater, and thus in anything that comes from the soil or the sea. And because it accumulates in living tissues, it can build up over a lifetime, which means that levels increase dramatically with each step up the food chain—part of why the FDA recommends that children and women who are pregnant or breastfeeding limit their consumption of large, carnivorous fish like tuna.1 But not all mercury is created equal: Some chemical forms of the element are more toxic than others. The main form found in tuna, methylmercury, is among the most damaging. It’s absorbed into the bloodstream more easily than other forms, and is harder for the body to clear. In the early 1980s, however, scientists studying what happens to mercury in the body when it’s ingested discovered that mammals have a remarkably powerful defense against this natural poison: the microbiome.
The 1984 report of their findings was not met with fanfare or widespread attention, even within the scientific community—which at that point in time was only beginning to recognize the microbiome’s importance for whole-body health.2 But the more we learn about both the power and fragility of the microbial ecosystem within us all, the more apparent it becomes that these results have enormous implications, which could impact how we think about everything from antibiotic use to psychiatric health.
1By signing up, you consent to receive Seed emails.
To understand how your gut is involved in processing mercury, it’s helpful to look back at that aforementioned study. The research began by putting three groups of mice on three different diets—one on a standard “lab chow” diet as a kind of control, one on a diet of powdered milk, and one on a high-protein liquid diet.
To study how mercury was absorbed and distributed throughout the animals’ bodies, the scientists then dosed them with radioactive versions of mercury-containing compounds. While that sounds extreme, it’s common practice in pharmacology studies: This kind of radioactivity isn’t enough to substantially change the toxicity or other properties of the chemical—it simply makes it easier to track and quantify. By comparing the radioactivity level of a fecal sample, urine sample, or tissue sample to the radioactivity in of the original dose, it’s possible to obtain a precise picture of what fraction of that dose ended up in a given waste product or body part. (This also helps avoid mistaking mercury that’s incidentally found in the diet for stuff administered as part of the study.)
Tracing the methylmercury over the following days, the research team found that diet had a huge impact on the animals’ ability to excrete it. Six days later, more than half the original dose had been recovered from the feces of the mice on the high-protein liquid diet—meaning it was safely out of the body, and was likely never even absorbed to begin with. In mice on the powdered milk diet, on the other hand, more than 80% was still found in the body, while the standard “lab chow” mice fell in between the other two groups.
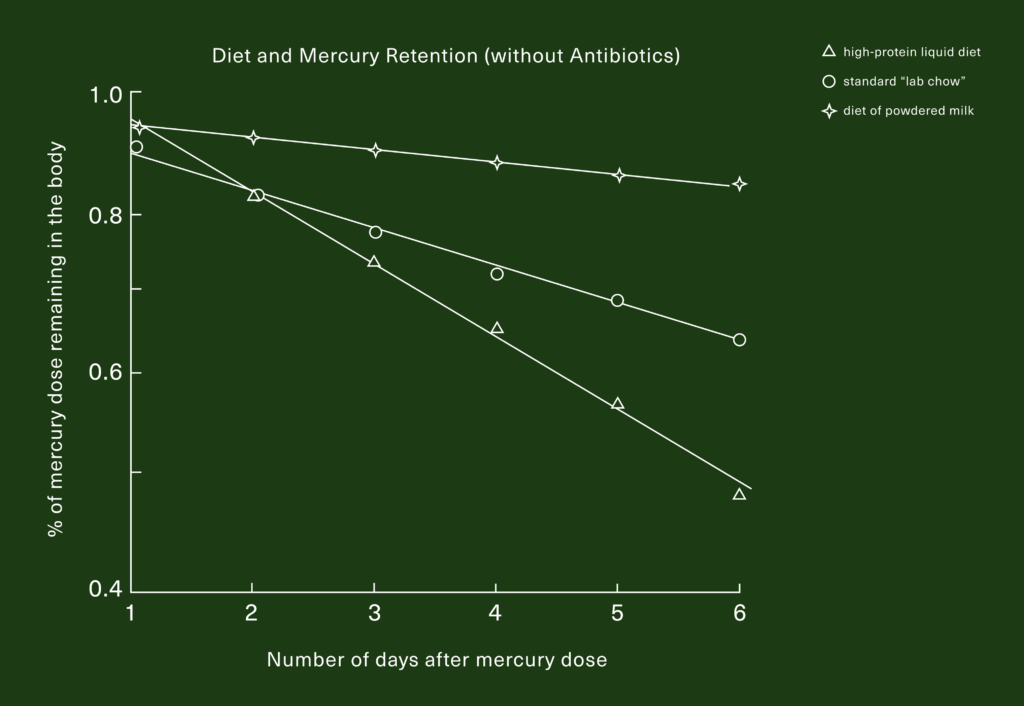
The lines on that graph are more or less straight, which makes it easy to assume that it’s only a matter of time before the amount of mercury remaining in the body goes to zero, regardless of diet—but that’s not the case. Once mercury is absorbed through the gut wall and deposited in tissues, it gets stuck to proteins. This is part of how it exerts its toxicity, and this stickiness makes it very difficult for the body to clear it. As a result, the first few days are the most critical in determining how much of any dose of mercury the body retains. If the experiment had been continued, the lines in the graph would likely plateau after the first few days, rather than continue pacing to zero.
This finding came as something of a surprise, particularly for researchers who study the gut. These experts might expect that a diet high in fiber would be the best for mercury elimination, since more fiber means more (and bulkier) poops, which could help carry the mercury out of the body. But both the best and the worst diets for mercury-elimination had practically zero fiber in them. Intrigued, the researchers suspected that the microbiome (then called “gut flora”—the word “microbiome” wasn’t coined until relatively recently) might be involved.
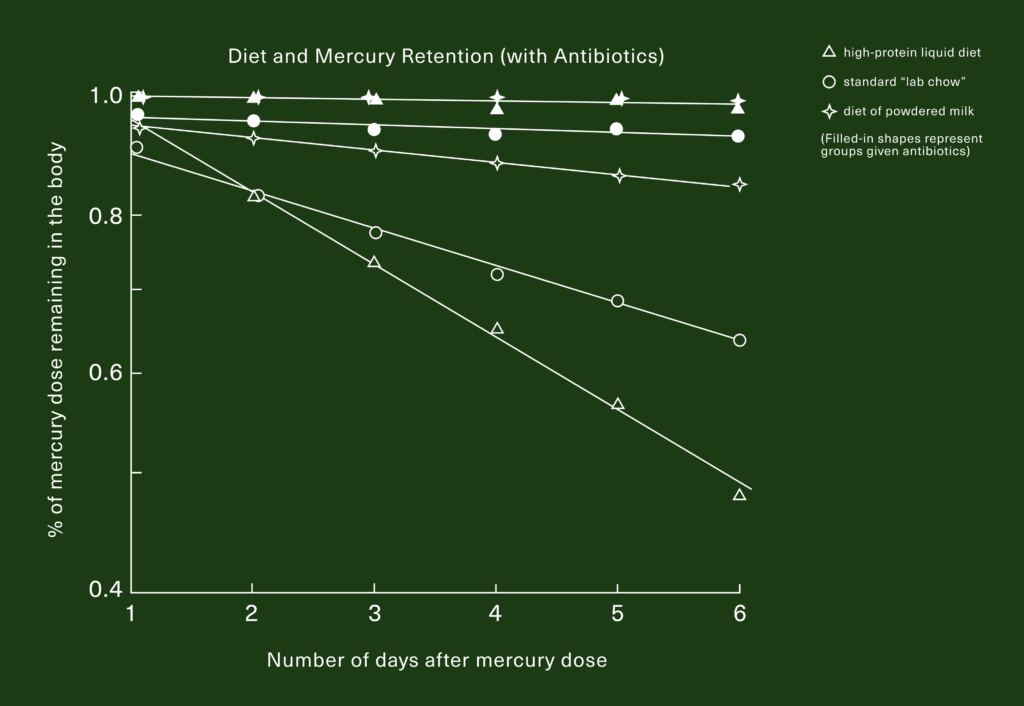
To test this hypothesis, they repeated the experiment with another three groups of animals, but gave them each a daily dose of antibiotics to wipe out their gut bacteria. If the first result had been a surprise, this one was downright startling.
When the mice were given antibiotics, it didn’t really matter what kind of diet they were on: Nearly 100% of the mercury they were fed stayed in their bodies.
This study was conducted in mice, but a similar study in rats found the same effect, and there’s little reason to think these findings wouldn’t apply to humans as well.3 The most important implication of this research is that gut bacteria can protect us from dietary heavy metals like mercury by trapping it in the GI tract, chemically transforming it in ways that prevent it from being absorbed into the body, and enabling us to excrete it in feces.
But it seems it’s only certain kinds of gut bacteria that do this. Which ones? It’s hard to say from these results, but there are hints. For instance: Milk sugars are great food for certain microbes like Lactobacillus and Bifidobacterium, but not so much for other species common to the microbiome. The fact that milk-fed mice do a really poor job of eliminating dietary mercury suggests that these aren’t the major players in protecting the body against it. This makes intuitive sense in terms of the role these microbes play in encouraging healthy development. In nature, mammals drinking milk are too young to be eating other foods, and the mother’s body already provides a layer of protection, filtering out most of the mercury from her diet in the process of turning some of the nutrients she eats into milk—meaning that nursing infants are generally exposed to less mercury, and therefore don’t need as much bacterial protection from it. The distinguishing feature of the best mercury-protective diet was its high concentration of easily digestible protein, which is promising in and of itself: If protein is what feeds mercury-trapping microbes, it’s lucky that most dietary mercury tends to be found in high-protein foods.
Another clue comes from a more recent study, which examined how the microbiomes of people from three different regions in China interacted with methylmercury.4 The research found that the abundance of bacteria from the genus Desulfovibrio, as well as the abundance of Archaea (the relatively mysterious “third kingdom” of life) were associated with a greater ability to transform methylmercury into less bioavailable—and thus less toxic—forms.
The crucial takeaway from all of this research is that antibiotics can drastically increase your body’s susceptibility to dietary mercury. Studies have shown that disturbances to the microbiome caused by a course of antibiotics can take three weeks or more to normalize5—so if you have to take antibiotics, it might be a good idea to lay off the tuna salad or mahi mahi for a few weeks afterwards, especially for pregnant or nursing women, and young children who are especially susceptible to the brain damage the metal can cause.
High-fructose corn syrup (HFCS) is another source of mercury in the diet that was only recognized relatively recently.⁶ The process of turning corn into HFCS involves some serious chemistry, and some of these chemicals can be produced using mercury—which eventually ends up in the corn syrup at concentrations of 0.2 to 0.3 ppm. Gram per gram, this puts HFCS somewhere between #9 and #10 on the list of high-mercury foods.⁷ However, the fact that HFCS is consumed in far greater quantities (the average American consumed more than 23 lbs of HFCS in 2021) means that it may be a major contributor to people’s mercury exposure total.⁸
But it’s also known that antibiotics can wipe species and genes out of a person’s microbiome entirely. If this happens, it can be hard to get them back—so perhaps the most intriguing possibility raised by this research is the notion that a disrupted microbiome could semi-permanently cause someone to lose the ability to excrete any of the mercury they eat. If this happened during a developmentally critical time period like early childhood, the effects could be devastating to a person’s course of neurological development.
It’s well known that the syndrome of social deficits caused by mercury toxicity, coupled with the ongoing rise in the prevalence of autism spectrum disorders, is part of why many people are skeptical of the safety of vaccines—despite the fact that most modern vaccines contain no mercury at all, and those that do contain it have less mercury per dose than is found in a single can of tuna.9 Nevertheless, a 2017 meta-analysis of 44 studies showed that people with autism spectrum disorders genuinely do have significantly higher levels of mercury in their blood and brain tissue compared to their neurotypical counterparts.10
While autism is a complex spectrum of conditions, gastrointestinal issues are a major component for a lot of people. Individuals with autism are significantly more likely to have functional gastrointestinal disorders than their neurotypical peers.11,12 And in light of the 1984 study, these facts begin to form the outline of a coherent theory: Maybe mercury is responsible for some subset of autism spectrum disorder (ASD) symptoms, but not as the result of increased exposure from vaccines. Instead, as the authors of the 2017 meta-analysis suggest, what if it’s a problem with the molecular machinery that’s supposed to help the body handle the mercury that we’re exposed to in the diet? The fact that our first line of defense against mercury is found in the microbiome—and is thus susceptible to disruption by antibiotics, diet, and other factors—means that a level of mercury exposure which is safe for one person could be toxic to another, depending on the composition of their individual microbiome. It also suggests the potential for new and exciting strategies to intervene when people have lost these genetic pathways—though that science is much more nascent.
So what does this all mean for you now? First and foremost, it’s a clear reason to practice caution when considering elective oral antibiotics (i.e., antibiotics that are not absolutely necessary). Sometimes, this can be as simple as an informed conversation with your doctor or primary care provider. Ear infections, for example, can often be treated equally well with antibiotic pills—which act throughout the entire body—or with antibiotic ear drops, which help avoid unnecessary collateral damage to the gut microbiome.13
Fish is still thought to be the primary source of mercury in most people’s diets—so if you have to take antibiotics and want to reduce the amount of mercury you’re consuming, the U.S. Food and Drug Administration has a handy chart for helping decide which fish should be avoided and which ones make good substitutes (it’s meant for children and those who are either pregnant, planning to become pregnant, or are breastfeeding, but it can still help you make more informed decisions). Additionally, the science around high-fructose corn syrup (HFCS) as a potential source of mercury exposure is relatively new, and isn’t taken into account by FDA guidelines—so it’s likely a good idea to cut as much HFCS as possible out of your diet when your microbiome has been compromised by antibiotics.
As of yet, there’s no probiotic you can take that will improve your body’s ability to excrete mercury, but the field of microbiome science is still very much in its infancy. As the science continues to develop over the next few years, a probiotic that helps protect us from environmental toxins is just one of the incredible technologies we might see on shelves. Watch this space—and mind your mercury intake in the meantime.

When you drink alcohol, your body embarks on a hero's journey to overcome the effects of imbibing. Here's how alcohol affects the microbiome and how you can support your gut in its fight to recover.
Transit time can be an illuminating data point about your digestive health. Here’s how to find out where you currently stand.

The new science of the microbiome suggests that we may have been thinking about dieting and body size all wrong.