Next Article
What Is Poop?
6 minutes
Transit time can be an illuminating data point about your digestive health. Here’s how to find out where you currently stand.
Your digestive system is designed to give you feedback. Experiences like bloating, upset stomach, diarrhea, and vomiting are just a few ways that your body “talks” to you about what’s going on as you digest. But your body uses other modes of communication that aren’t as clear-cut to discern—unless you’re looking for them.
One way to glean information from your digestive system is to figure out how long it takes for food to go from your mouth all the way through its eventual exit—your rectum and anus. And there’s actually a scientific unit for this: It’s called “Whole Gut Transit Time.” Here, we’ll explain what it can tell you about your body (and your gut microbiome), and how to measure your transit time at home.
“Whole Gut Transit Time” (aka WGTT, or simply “transit time”) refers to the amount of time from when you initially eat a food to when you poop that food—well, remnants of it—out.
Studies suggest that the median WGTT is about 28 hours, and it’s considered “normal” for an individual person’s transit time to fall between 10 and 73 hours.1,2 That significant range accounts for what you’ve eaten and how much, as well as individual factors like your age, sex, stress levels, medications, colon anatomy, hormones, diet, and, of course, the gut microbiota (the microorganisms in your gastrointestinal system) and its metabolites (what those microorganisms produce).3
Also, it’s worth noting that WGTT varies significantly not only between individuals, but also within individuals day to day. So you don’t have a singular, fixed transit time, as it can fluctuate throughout your life depending on the aforementioned factors.
At this point, you might be wondering: When you take a bite of food, where exactly does it go for ~28 hours? From the outside, it may not seem like your food has to take a long journey to get through your digestive system. But looks are deceiving: A 2002 study4 examined the length of the entire intestinal tract in 100 women and 100 men and found the average length for females was 7.54 meters (24.7 feet) and for males it was 8.37 meters (27.5 feet). Additionally, a 2014 study5 likened the total surface area of your intestines—laid out flat—to about half the size of a badminton court (22 feet). And it’s all scrunched into the area between your mouth and your anus.
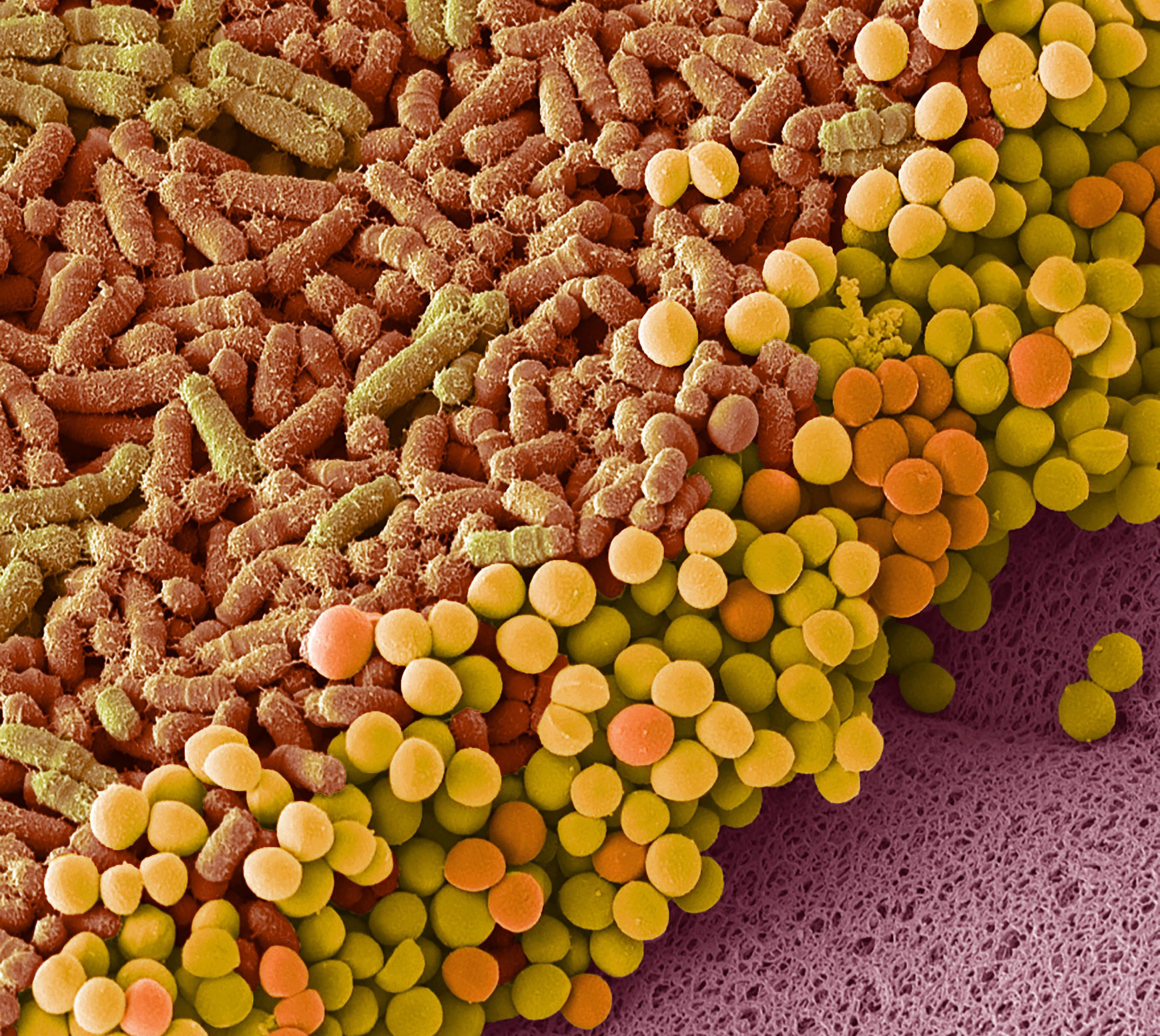
The journey of digestion starts in your mouth, continuing through the esophagus, stomach, small intestine, large intestine (colon), rectum, and anus. Together, these make up your gastrointestinal (GI) tract—the part of your body that plays host to all the inputs passing through (foods, liquids, air, medications), as well as an estimated 36 trillion resident bacteria that live within.6
As food travels along this pathway, it’s broken down mechanically (via chewing and muscular contractions), chemically (via digestive enzymes and stomach acids), and by the microbiota in our gut, metabolizing macronutrients and fermenting non-digestible fibers.7 Once your food reaches its final destination (i.e., the toilet), it’s almost completely unrecognizable from your initial bite.
Studies have found a connection between WGTT and the gut microbiome function.8 While that relationship is complex and still requires further research, it is clear that the association between your gut and your transit time is a two-way street, so to speak. The gut microbiota directly impact transit time by producing metabolites that stimulate motility, the process by which muscles contract throughout your digestive tract to move food and waste through your system. In turn, transit time can impact the gut’s microbial composition and metabolism.7,9 Scientists currently have a good understanding of how the former connection works, and less of how the latter works. Meaning: How your gut bacteria impact transit time is better understood than vice versa.
So what does it mean when your transit time is relatively slow or fast?
To answer that question, it’s helpful to understand the mechanism by which your gut bacteria impact transit time. Gut bacteria tend to use carbohydrates as a primary source of energy.9 As they consume these carbohydrates, they create beneficial byproducts (i.e., metabolites), that not only influence transit time, but support and strengthen the gut barrier and help support the immune system.10
With a slow transit time, bacteria may be deprived of carbohydrates to consume and start to feed on protein instead.11 Byproducts made from the breakdown of protein, such as ammonia and sulfur compounds, can have harmful effects12,13 on gut and metabolic health—for example, increased mucosal damage3, disruption of colon cell tight junctions, and increased inflammatory response.14 (It’s also worth noting that the slower material passes through the colon, the more water is drawn from stool, which makes it harder to pass and can cause issues like constipation.)
On the other hand, if food passes through too quickly and transit time is relatively fast, you may not absorb the optimal amount of nutrients. This, along with dehydration, is one of the main concerns with a chronic fast transit time. Digested food material needs to spend enough time in the GI tract to absorb water and nutrients properly. Certain health conditions can also result in a faster-than-average transit time.15,16,17
Of course, transit time is just one data point of many when it comes to your gut health. Given that your transit time can change on a daily basis, it’s not meant to be an at-home diagnostic tool. If you’re at all concerned about your transit time, it’s always a good idea to talk to your doctor.
Interested in doing your own personal study? You can perform an at-home experiment to measure your current transit time. One method we like is the corn test. Here’s how it works:
It’s not a perfect measure of WGTT, but it will give you a good approximation of where you stand.* And if you’re wondering, Why corn? Corn is actually a seed protected by a tough outer shell that’s made of cellulose. Our bodies don’t have the proper enzymes to break down and digest cellulose, so this outer shell passes right through us and can be seen speckling our poop. You might even say that corn kernels are the “Big Dipper” of stool-gazing.
*Disclaimer: We do not recommend this experiment if you have difficulty swallowing, pre-existing GI conditions, or are allergic/hypersensitive to corn. This experiment is not intended to diagnose any medical conditions nor is it a substitute for professional medical evaluation. If you have any questions or concerns, please consult your primary health care provider. Children should not participate without adult supervision.
At the end of the day, transit time is just one piece of information if you’re investigating your bowel movements. Whatever your situation, here are some evidence-based tips to support easy poops:
Citations:
Transit time can be an illuminating data point about your digestive health. Here’s how to find out where you currently stand.

Strategies for supporting digestive health beyond diet—from regulating your sleep timing to exploring your local park.

Exactly what Seed's Chief Medical Officer looks for (and avoids) when identifying high-quality probiotics.