Next Article
How Microbiome-Informed Treatment Could Revolutionize UTI Care
6 minutes
Treating a vaginal infection is not the same thing as curing it. While antibiotics can treat initial vaginal infections, they can make the vaginal microbiome more susceptible to follow-up problems.

If you just can’t seem to escape vaginal infections, even after taking antibiotics, you’re not alone. Check any vaginal health message board and you’ll hear from people who have suffered from seemingly treatment-resistant issues like bacterial vaginosis (BV) and yeast infections for months, years, or even decades. Many have tried all types of over-the-counter and prescription medications to cure their abnormal vaginal discharge, odor, and discomfort to no avail. This leads to feelings of immense frustration, embarrassment, and shame, with many women reporting feeling “broken” and desperate to try anything—even dubious DIY remedies—in order to “fix” themselves.
Their accounts are wildly upsetting, and they show that treating a vaginal infection is not the same thing as curing it. While antibiotics often work for initial infections, they can also shift the vaginal microbiome in a way that increases susceptibility to subsequent problems. It’s time to uncover the root cause of vaginal infections in the name of real, lasting relief.
1By signing up, you consent to receive Seed emails.
The cause (and oftentimes, the cure) of many vaginal infections lies in the vaginal microbiome (VMB). Just like your gut, your vagina is home to an ecosystem of microscopic residents. Ideally, these microbial communities protect the vaginal environment from invaders.1
Throughout your life, the microbes residing in your vagina will shift. These changes in VMB composition are common, normal, and not at all “your fault.” Everything from your menstrual cycle to your pregnancy status to the types of period and personal care products you use can alter the composition of your VMB, at least temporarily.2,3 Oftentimes, these fluctuations are unnoticeable, but sometimes, they can lead to a microbial imbalance or decreased ability to fight off infection.
In general, there are two categories of infections that can impact vaginas. The first is an imbalance in the microorganisms that naturally populate the vagina, which can cause (extremely common and not at all shameful) issues like BV.
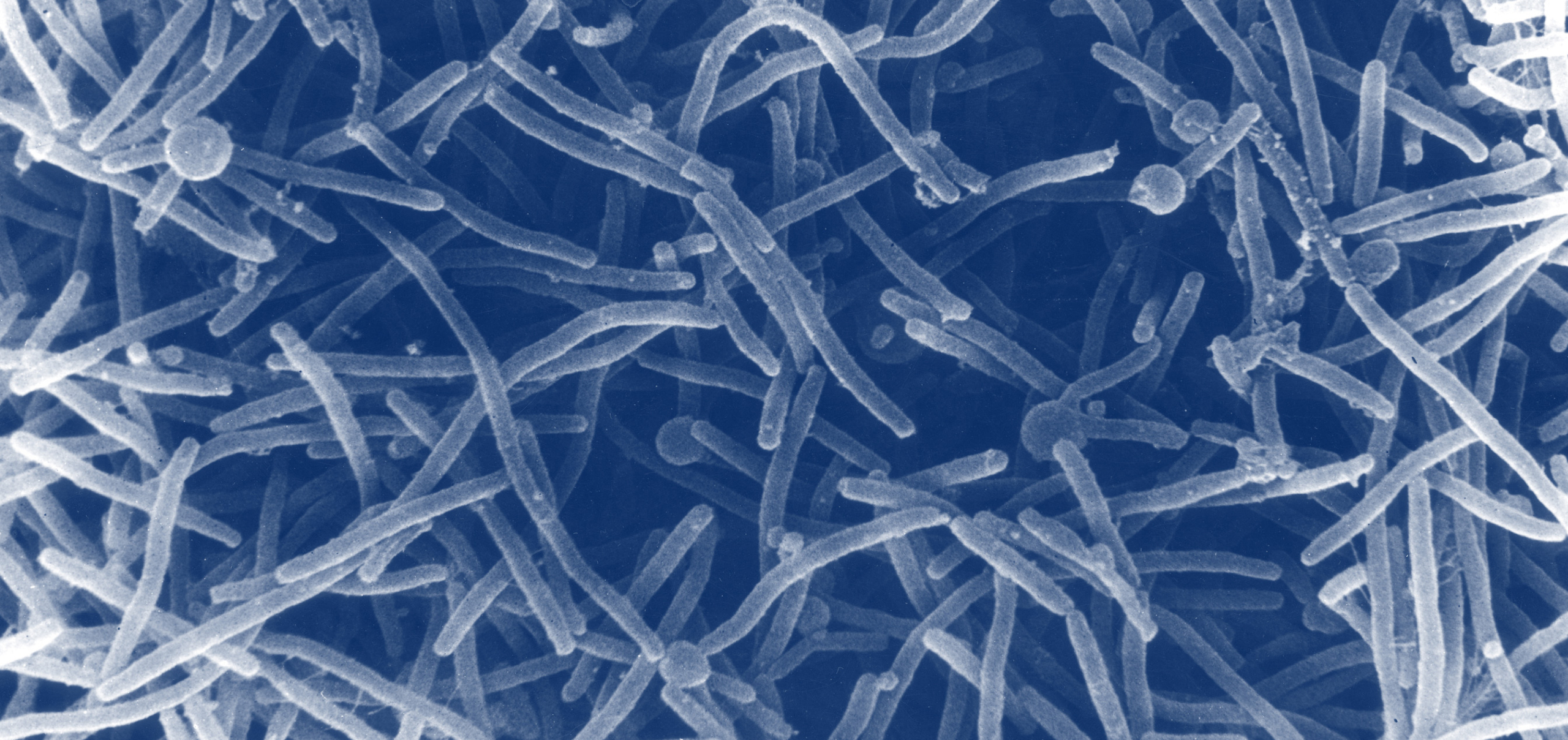
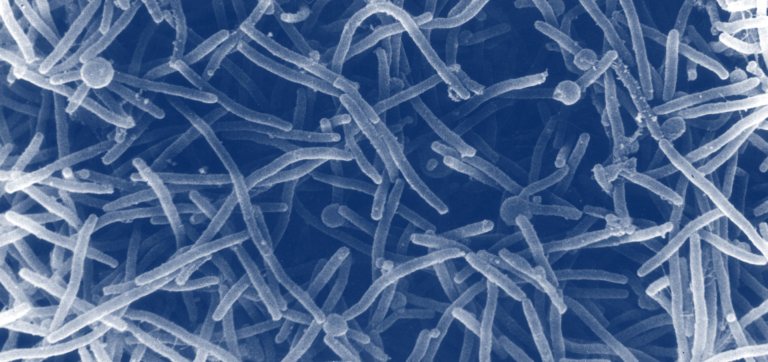
It’s estimated that nearly one-third of reproductive-aged women have BV at any given time—meaning women are more likely to have BV than have blue eyes in this country.4,5 BV occurs when microorganisms that are typically less abundant in the VMB, such as Gardnerella vaginalis, Atopobium vaginae, or Ureaplasma urealyticum, grow to become more prominent than protective bacterial species like Lactobacillus.4,6
BV is usually accompanied by a shift in the pH level of the vagina. Ideally, the VMB maintains a moderately acidic vaginal environment (between 3.8–5.0 during non-pregnant reproductive years), which is optimal for keeping potentially harmful bacteria at low levels. However, when BV occurs, vaginal pH becomes less acidic, creating an opportunity for pathogens to grow and thrive.7
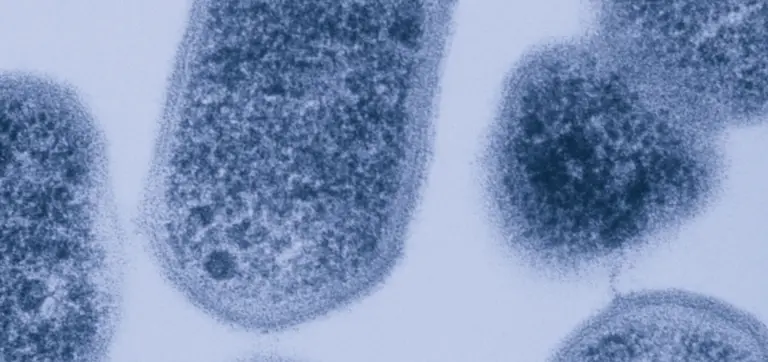
The second category of vaginal infection occurs when microbial pathogens are introduced into the vagina from a sexual partner. Chlamydia, caused by the bacteria Chlamydia trachomatis, is the most frequently reported bacterial sexually transmitted infection (STI) in the U.S.8
Once Chlamydia trachomatis enters the body, it adheres to and penetrates cells lining the vagina, where it can evade immune attack and replicate. Vaginal microbiomes that contain species of bacteria such as Lactobacillus crispatus and Lactobacillus jensenii have been shown to actively protect against chlamydia infection, likely due to the forms of lactic acid they produce.9
“Some naturally occurring vaginal microbes are better suited to protect against chlamydia,” Jacques Ravel, Ph.D., a leading expert in vaginal microbiome science, explains.
To treat bacterial infections like chlamydia and BV, most doctors will prescribe a round of antibiotics.
The most common treatments for BV are metronidazole or clindamycin antibiotics, which can be taken orally or vaginally.4 These treatments have been shown to reduce harmful bacteria in the vagina. However, Dr. Ravel notes that they do nothing to rebuild a strong and resilient VMB post-infection. He adds that antibiotics that broadly target all microbes may also “decrease the overall abundance of microbes in the vagina, which can leave open a gap for new invaders to take advantage of.”
You can think of antibiotics like pesticides: They do a great job at clearing fields of harmful pests, but they also get rid of beneficial bugs, and they don’t do anything to enrich the soil itself. It’s not surprising, then, that studies demonstrate over 50% of women who take antibiotics for BV have a recurring infection within three to six months.10
Chlamydia return rates tell a similar story. The infection is often treated with antibiotics including azithromycin or doxycycline and around 25% of women treated will have a repeat infection. These could be caused by remaining remnants of the initial infection, resistance to the original antibiotic used, or a reinfection by a new strain of Chlamydia trachomatis.11
Beyond allowing recurrent infections, some antibiotics can also make women more susceptible to a vaginal yeast infection, or vulvovaginal candidiasis (VVC).12
“There are cases where a woman may take an antibiotic for another issue, then a yeast infection follows,” Dr. Ravel says, noting that this can happen when antibiotics deplete the microbiome of protective bacteria and create an opportunity for new yeast to grow or existing yeast to multiply.
Dr. Ravel, who has conducted many vaginal microbiome surveys, says that “about 20% of women have naturally occurring Candida yeast in the vagina but are asymptomatic.”13 This means that roughly 1 in 5 women are unknowingly dependent on a protective bacteria in the VMB to keep their yeast at a low level. However, this delicate balance can easily become skewed when antibiotics come into the picture.
Case in point: recurrent vulvovaginal candidiasis (RVVC), defined as three or more episodes of VVC a year, is now estimated to cost the United States healthcare system over two billion dollars annually because it’s so difficult to treat.12,14
Antibiotics taken for other issues that have nothing to do with the vagina can also throw off the VMB in ways that make it more susceptible to bacterial or yeast infections. Let’s say, for example, you have an infection in your throat and you take a prescription antibiotic orally for one week. That antibiotic will go through your digestive system and get absorbed into your bloodstream to be transported all over the body—including to the vagina (hence why oral antibiotics are often prescribed for vaginal infections), where it can alter your VMB.11,12,
This isn’t to say we should give up on antibiotics completely. In many cases, they’re necessary and even life-saving. However, the research is clear: we need to start using them in a way that minimizes microbial disturbance.
Dealing with occasional vaginal irritation is one thing. Suffering through multiple infections a year and facing chronic vaginal pain, malodor, or abnormal discharge, is quite another. In addition to causing uncomfortable physical symptoms, common (and too-often-stigmatized) vaginal conditions can negatively affect self-esteem, quality of life, and relationships. It’s past time to do something about them.15
Dr. Ravel emphasizes that the medical community needs to shift their use of antibiotics and pair them with microbiome protections. Ava Mainieri, Ph.D., a geneticist and evolutionary biologist specializing in female reproductive health, agrees, adding that women can also proactively protect their microbiome before, during, and after a round of these medications. This can look like taking a vaginal probiotic containing strains that are native to the vagina, avoiding microbe-disrupting practices like douching or using feminine washes, and practicing safe sex.3,7 If you’re dealing with a persistent or recurrent vaginal infection, be sure to consult with your healthcare provider for personalized guidance on how to prevent future episodes.
While antibiotics are indisputably necessary, research shows that in the long run, women need more—more compassion, more respect, and a more proactive approach that ensures lasting relief.


From douching to smoking, here are the known triggers of vaginal dysbiosis and how to overcome them to get your microbes back on track.
What exactly is bacterial vaginosis? What causes it? And how can you treat it so it doesn’t come back? We answer all of it and more in this shame-free guide to BV.
Chances are, you’ve never heard of the urobiome—but it could hold the key to more effective UTI treatment and prevention.